

 ไทย
ไทย
This article presents the success story of Ms. Mint (33 years old), who experienced infertility due to Polycystic Ovary Syndrome (PCOS) and underwent ICSI treatment at LRC Fertility Clinic. The case highlights the effective use of the Antagonist Protocol, which resulted in a high blastocyst development rate. This case demonstrates the importance of accurate diagnosis, personalized treatment plans, and advanced laboratory technology in enhancing the chances of pregnancy for PCOS patients
Case Background
- Primary Physician: Somphoch Pumipichet M.D.
- Case Type: PCOS (Polycystic Ovary Syndrome) – Antagonist Protocol with a High Blastocyst Development Rate
Female Patient Information: Ms. Mint (Pseudonym)
- Age: 33 years old
- Pregnancy History: One child, seeking a second pregnancy
- Medical History:
- Polycystic Ovary Syndrome (PCOS)
- Issues with imbalanced follicular development and chronic anovulation
- Ovarian Condition at the Start of Stimulation:
- Antral Follicle Count (AFC): 17 follicles (7 on the right, 10 on the left)
- LH (Luteinizing Hormone): 15.80 mIU/mL (Significantly higher than normal, indicating a risk of premature ovulation)
- E2 (Estradiol): 47.60 pg/ml (Ovaries still have good reserve, but hormone levels are imbalanced)
Ms. Mint and her husband came to LRC Fertility Clinic with the desire to have a second child. Given her age and limited time, they decided to pursue assisted reproductive technology at 33, which is still a relatively optimal age. However, Ms. Mint had been suffering from PCOS for a long time, which not only led to uneven follicular development but also posed a risk of reduced egg quality.
Challenges in Ms. Mint’s Pregnancy Journey
For PCOS patients, a high LH level requires extreme caution during ovarian stimulation. Excessively high LH can lead to premature luteinization or premature ovulation, directly impacting the number of retrieved eggs and the rate of mature egg development. Concurrently, although PCOS patients often have a high antral follicle count, follicular development is often inconsistent. Therefore, ensuring synchronous follicular development and improving egg quality are crucial for success. Fortunately, Ms. Mint’s other baseline indicators were within good ranges, providing a solid foundation for subsequent treatment.
Treatment Plan
Given Ms. Mint’s specific situation, an experienced physician, Somphoch Pumipichet M.D. from LRC Fertility Clinic, designed a delicate and precise personalized treatment plan. Before starting ovarian stimulation, Dr. Sompoch Phoomphichen established a hormone balancing plan aimed at normalizing Ms. Mint’s hormone levels, specifically reducing abnormally high LH, and focusing on improving the quality of potentially problematic follicles. For the ovarian stimulation protocol, the Antagonist Protocol was chosen due to its flexibility and ease of control, allowing for timely medication adjustments based on follicular response and hormonal changes during the treatment cycle.
The ovarian stimulation cycle began on day 3 of her menstrual period. During stimulation, close monitoring was conducted through frequent transvaginal ultrasounds and detailed hormone level measurements. Dr. Sompoch’s medical team closely observed Ms. Mint’s response at every step.
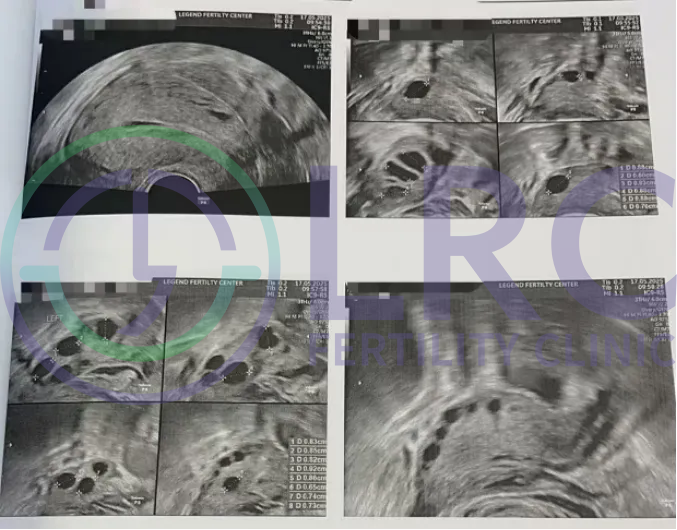
Day 3 of Menstrual Cycle (Start of Stimulation):

- Ultrasound: 17 antral follicles (Right: 7 follicles, sizes 6, 6, 6, 6, 6, 6, 6 mm; Left: 10 follicles, sizes 6, 6, 6, 6, 5, 5, 5, 5, 4, 4 mm)
- Hormone Levels:
- FSH (Follicle Stimulating Hormone): 15.80 mIU/mL
- E2 (Estradiol): 47.60 pg/ml
Day 4 :
- Ultrasound:
- Right: 7 follicles (sizes 9, 9, 9, 8, 8, 7, 7 mm)
- Left: 10 follicles (sizes 10, 9, 9, 9, 8, 8, 8, 8, 6, 6 mm)
- Hormone Levels:
- LH (Luteinizing Hormone): 8.8 mIU/mL
Day 6 :

- Ultrasound:
- Right: 10 follicles (sizes 14, 13, 13, 12, 12, 11, 9, 9 mm)
- Left: 12 follicles (sizes 14, 14, 13, 13, 12, 12, 11, 11, 11, 9, 8, 8 mm)
- Hormone Levels:
- LH (Luteinizing Hormone): 6.2 mIU/mL
- E2 (Estradiol): 843.2 pg/ml
Day 8 :
- Ultrasound:
- Right: 11 follicles (sizes 17, 17, 17, 17, 16, 12, 12, 12, 11, 10, 10 mm)
- Left: 12 follicles (sizes 17, 16, 16, 15, 15, 14, 14, 13, 12, 11, 10, 10 mm)
Day 10:

- Ultrasound:
- Right: 11 follicles (sizes 18, 18, 18, 17, 17, 14, 14, 14, 13, 13, 12 mm)
- Left: 11 follicles (sizes 20, 19, 19, 18, 18, 17, 17, 17, 17, 16, 16 mm)
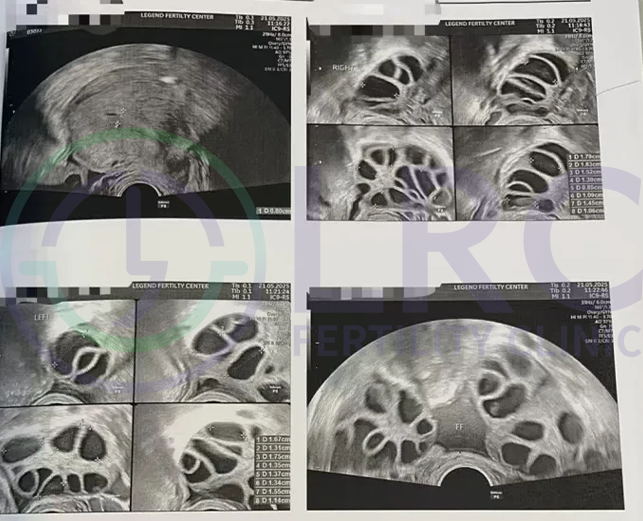
Day 11 :

- Ultrasound:
- Right: 14 follicles (sizes 21, 20, 20, 21, 19, 19, 19, 18, 18, 18, 17, 16, 15, 14 mm)
- Left: 14 follicles (sizes 22, 20, 20, 20, 20, 20, 19, 19, 18, 17, 17, 17, 17, 16 mm)
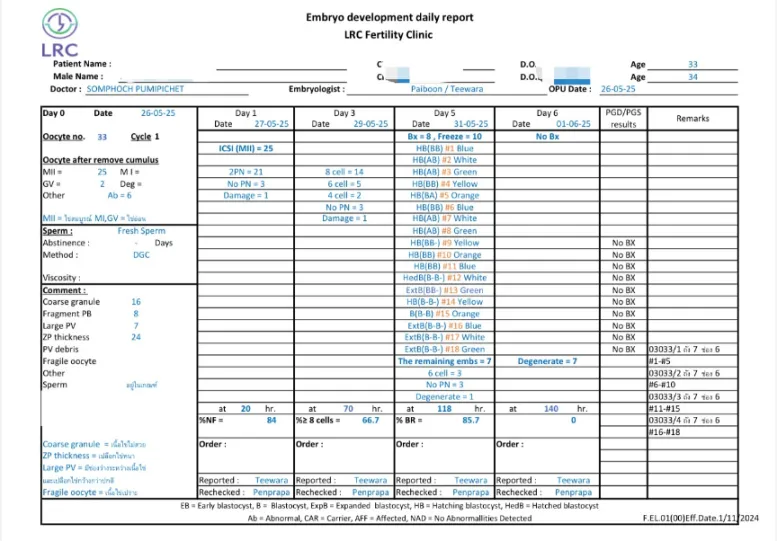
Egg Retrieval, Fertilization, and Embryo Culture Results
- Number of Eggs Retrieved: 33
- Mature Eggs (MII): 25
- Eggs Fertilized by ICSI: 21
- Number of Successful Blastocyst Embryos: 18
Blastocyst Development Rate: 86%
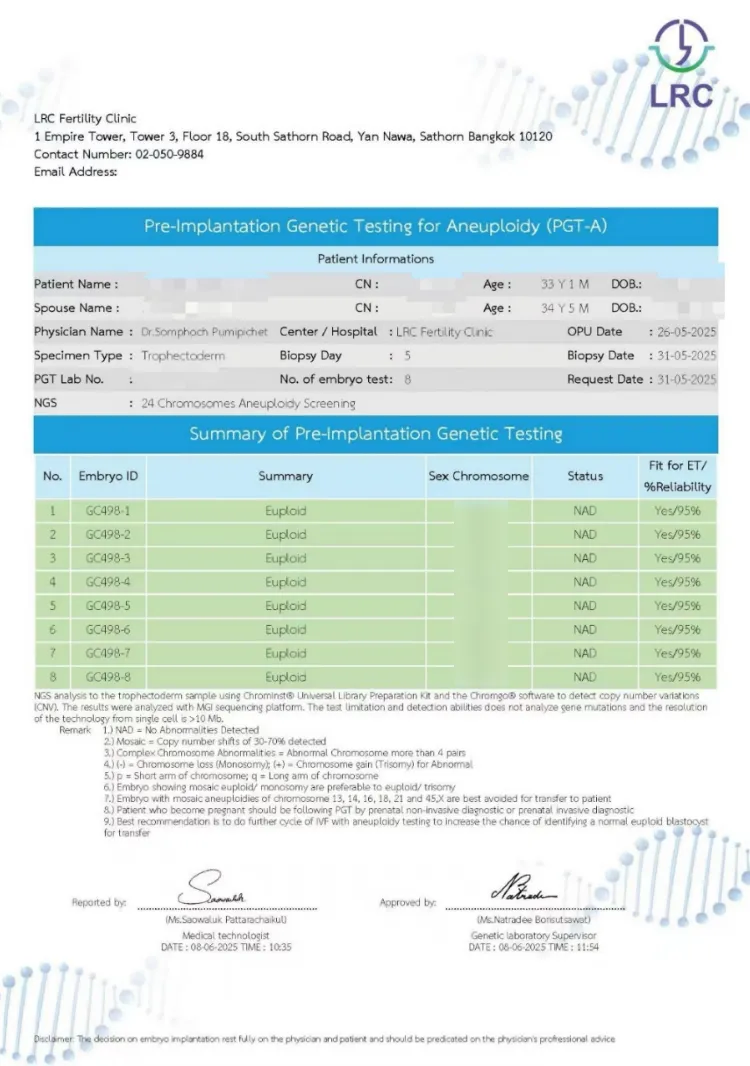
PGT-A Chromosomal Screening Results
- Blastocysts Sent for Testing: 8
- Blastocysts that Passed Screening (Suitable for Transfer): 8
- Screening Pass Rate: 100%
Key Takeaways and Treatment Summary
Key Takeaways from the Case:
- Personalized Treatment Design: For complex cases like PCOS combined with abnormally high LH, LRC Fertility Clinic’s medical team, led by Somphoch Pumipichet M.D., precisely planned the preparation and ovarian stimulation. The dynamic adjustment of the plan effectively avoided risks.
- Meticulous Ovarian Stimulation Planning: Through close monitoring and continuous medication adjustments, follicular development progressed uniformly, maximizing the egg retrieval rate and egg quality. Not a single valuable egg was lost.
- Expertise of a Leading Embryology Laboratory: The high blastocyst development rate of 86% is strong proof of the embryology laboratory’s excellent technology, stable culture environment, and extensive experience, which allowed the embryos’ full potential to be unleashed.
- Comprehensive Infertility Treatment Model: Having a large number of high-quality blastocyst embryos provides more options for elective embryo transfer, planning for future pregnancies, and even fertility preservation.
Treatment Summary:
Ms. Mint’s case offers three crucial insights for patients with Polycystic Ovary Syndrome (PCOS):
- Seek Treatment at a Younger Age: The period before age 35 is considered the “golden window” for IVF. Ms. Mint decided to start ovarian stimulation at 33, which helped avoid the risk of age-related ovarian decline. Even PCOS patients with regular periods should assess their fertility early through AMH and 6-hormone tests and Don’t delay just because you “think you’re young.”
- Choose Appropriate Infertility Treatment: The primary challenge for PCOS patients is having many follicles but poor quality eggs. It’s essential to move beyond the limitations of traditional ovarian stimulation that solely focuses on quantity. The medical team performed pre-treatment hormone balancing and dynamically adjusted medication during stimulation, allowing previously erratic follicle growth to become uniform. This demonstrates that precise and personalized treatment is key to achieving pregnancy even with PCOS.
- Quantity of Eggs is Less Important than Quality: In this case, 25 mature eggs developed into 18 good-quality blastocyst embryos (an 86% rate). This is a result of advanced embryo culture technology. PCOS patients should not only aim for a large number of retrieved eggs but should also choose a clinic with a high-standard, independent embryology laboratory with extensive experience in embryo culture to increase the chance of successful pregnancy through high-quality embryo banking.
PCOS is not a dead end for having children. When a medical plan profoundly aligns with the patient’s specific characteristics, even complex cases with hormonal imbalances can unlock the full potential of each egg.